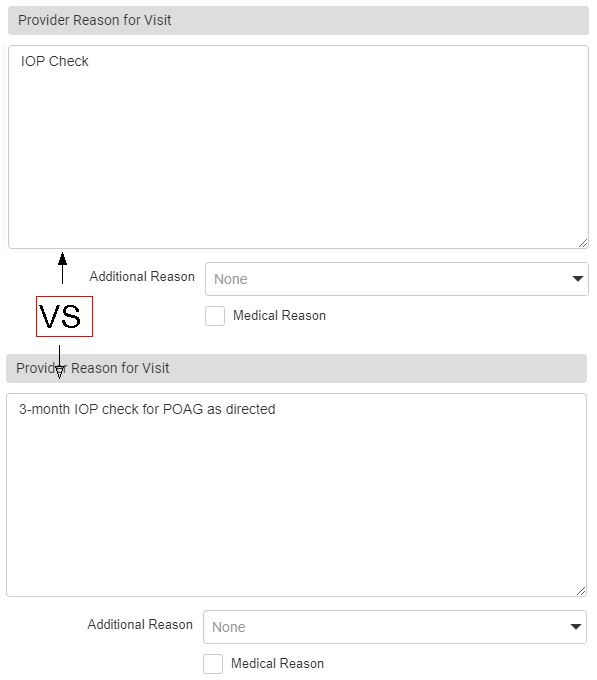
While frequently used by many providers, non-descriptive terminology within the medical record can create challenges in an audit. Consider a reason for visit of “IOP check” vs. “3-month IOP check for POAG as directed.” Both are correctly stating what the patient is in the office for today. But the latter provides a level of detail that cannot be challenged in an audit the way “IOP check” could be challenged. See Example
{kind=link}
As another example, providers will often conclude a care plan item with the term “Monitor.” It is quite easy to improve that by adding a quick reference to “when and why," e.g., Monitor for progression in 6 months.
Finally, it can be good practice to avoid standing orders such as “return annually for exam” or “repeat test yearly.” While there are certainly times that we practice with these notions in mind, the third party interpretation can be that these tests are going to happen in perpetuity irrespective of the patient’s clinical status. Each visit’s care plan should ideally be tailored to the needs of the patient based on that visit’s evaluation. Use of terms like “annually” and “yearly” provides an avenue for the third party to argue that tailoring is not happening.
Providing specifics about why a patient is being seen, why a test is being ordered, or when and why you would like to see the patient back does not need to be a laborious task. As you can see above, just a quick reference to those details will suffice and it will go a long way toward helping the medical record in third party review.